


Treatment vs. Healing
Life in the 21st C. Medical-Industrial Complex

This is the sequel to my hospitalization tale, containing both a chronicle of the weeks after my release from Kaiser and my thoughts regarding cardiovascular (CV) disease and how Western medicine deals with it. The tone will be different than my previous post. I remain very grateful that my encounter with the healthcare system turned out as well as it did. Even so, I believe ambivalence is the smart attitude to take when you see how it works (or fails to work) for vast numbers of people around the world.

In the Senior Care Home
I decided to transfer to a care home (at my own expense) in large part because Kaiser required me to have someone present to look after me for the first two weeks. Neither my friends nor my girlfriend, who had just arrived from Europe, could be expected to play the role of caretaker. Also, my flat was a less than ideal environment for someone healing from open heart surgery: two flights of stairs to reach the flat, plus very steep hills all around.
A senior placement agency lined up a few options, all of which were expensive (don’t compare it to a holiday resort, that way lies madness). The one I picked was not the cheapest deal, but it was in a familiar part of S.F. rather than a distant suburb, so my friends could visit easily. The two-story house was one of countless midcentury boxes made of ticky tacky, indistinguishable from its neighbors in the Sunset district, but modified to accommodate six residents and up to three staffers (Filipino, of course).
This arrangement is often called assisted-living. The care offered is not at the level of skilled nursing facilities. Most of the residents there were senescent and housebound, unable to feed or wash themselves — the kind who never appear in glossy brochures for senior communities. Their lives are spent vegetating in beds or in chairs, staring vacantly at TVs day and night, and being spoon-fed like babies.

As you might imagine, the prospect of two weeks of this memento mori was far from what I’d had in mind. But all I needed was my own room, three meals a day, laundry service, and attendants on-site. I could wash and dress myself and take my meds without supervision. At first it was hard to disengage myself from the plight of the other residents — it was very different than Kaiser Hospital. Here my condition was much closer to that of the staff. Along with Arthur, a retired dentist recuperating from an iatrogenic illness, I would soon leave under my own power. The rest were being kept in storage, waiting to die. They were the responsibility of the staff, who had to do the best they could in a situation they did not create.
At that time, a major improvement in my quality of life was simply being out of the hospital — it meant proper rest for the first time in weeks, sleeping in a normal bed, with no interruptions save mealtime announcements. I was given one of the five bedrooms on the ground level behind the garage. There was no lift, so I walked upstairs to take my meals with Arthur and the caretakers Bok, Ryan, and Joseph. The cuisine was often Filipino, which I might have deemed unsuitable for cardiac patients, but I was glad for the home style cooking and would take my chances for two weeks. Arthur and I, being acquainted with Hawaii, noted the overlap of Pinoy and Hawaiian dishes. Among our meals were such classics as menudo, pancit, adobo and lumpia. Not exactly heart-healthy, but satisfying. One day I had to laugh when Joseph served us fried eggs and Spam with rice, i.e., Spamsilog, Breakfast of Champions!

Aside from working out my lungs with an incentive spirometer, my daily exercise consisted on walking, first in the back yard, then in the neighborhood with one of the staff (or a visiting friend) as escort. The streets were mostly flat with gentle grades, so walking could be a challenge sometimes, but not too much as long as I paced myself. My bypass operation had become less of a concern — it only demanded my attention when I washed my incision scars, carefully peeling away bits of medical crazy glue. Instead I became more interested in my meds, as I was taking several (some only short-term) and the most obvious side effect was lightheadedness, reminiscent of jet lag. For sure it could’ve been worse. More on this subject anon.
As I rarely watched TV except for the one with Netflix in the living room, I had time to contemplate and educate myself about CV disease, the world’s leading cause of death (cancer is catching up). The contemplative part had to do with mortality. Thanks to medical advances and lifestyle choices, I had been given more time, and as I told my surgeon, I intend to use it well. If I have just ten good years left, that will have to be enough. It’s more than my father had; he died of a heart attack at sixty — back in 1971 the coronary bypass operation was not nearly as commonplace as it is today.
Gradually I got used to the routines. Washing myself in the chilly bathroom with a giant walk-in shower. Learning to climb in and out of bed safely with the least strain on my rib cage. Residents calling for the staff at night (we had no silent call buttons). Taking meds and vital signs. Walking, resting, and reading. Among the highlights: going with my girlfriend Julie to watch “Top Gun: Maverick” with the SF Symphony playing the soundtrack live; and a visit to Ocean Beach, where Arthur, Ryan and I walked along the Great Highway. For Arthur it was his first walk outdoors since being hospitalized last summer, so you can imagine his exultation.
I finished reading, “Finn Family Moomintroll” (Julie turned me on to Tove Janssen’s Moomins), then started researching atherosclerosis online in earnest. This subject, even pursued at layman level, is inexhaustible.
The Degenerative Disease(s)
Like virtually everyone of my acquaintance, I rarely gave chronic illness much thought — that is, until it became personal. Now that I have skin in the game, my perspectives on health and medicine (mainstream & alternative) have shifted a bit. In the Western allopathic tradition it is typical to divide the body into systems of components, much like a complex vehicle. Each system has an army of specialists to troubleshoot issues and offer relief by adjusting one’s settings or repairing worn or defective parts. This is not the same as healing or curing, terms that imply the end of a sickness and a return to health. What they offer is treatment, or management. This is not to be trivialized, for ex., pain relief, which doesn’t solve physical injury by itself, can play a decisive role in helping a patient get proper rest, so the body can heal itself more effectively.
As many of us have noticed, despite the vast amounts of data accumulated and the new drugs and technologies developed over the past century, millions worldwide continue to suffer and die from ailments which are treatable but incurable. If one takes the charitable view that the status quo is due to lack of knowledge rather than malicious intent, there is still far too much ignorance that conveniently generates massive profits for the medical-industrial complex. Factoring in the interests of the food and chemical industries, it becomes harder to distinguish collective stupidity from psychopathic greed. We definitely seem to have both working against us.
Looking at CV disease — in my case, atherosclerosis that manifested as coronary artery disease — often the condition goes undetected until it has advanced to a life-threatening stage. Ultimate causes remain murky; in fact the initial damage to our arterial linings (endothelial dysfunction) begins in childhood. One study suggests that early trauma is one of the factors leading to CV disease in midlife. Is there anyone who hasn’t suffered trauma as a child? It’s quite a different picture than what we’ve been told, i.e., lower your blood pressure and cholesterol, and here are the drugs to do it. This is because our medical system only really informs us about the symptoms or risk factors that it can adjust easily. It’s not here to fix the world.
Childhood Trauma and Cardiovascular Risk
Perhaps this is simply the price of admission to this wretched simulation. “You wanna play the game as a human? Here’s your trauma! Next!”
The damage started long ago, and for whatever reason the body’s attempts to repair itself are just not good enough. The patch (i.e., plaque) in the artery bulges inward, restricting blood flow, and it just worsens over time. Are there no examples of a smooth arterial repair in nature?? Some of us also suffer an innate disadvantage from producing excess cholesterol, which can be an inherited trait (like multigenerational trauma, perhaps?) Rest assured that gene therapy is being developed right now to remedy familial hypercholesterolemia (for the adventurous among us).
To Infinity and Beyond
At some point a comprehensive view of the medical-industrial complex must include Transhumanism. The concept deserves analysis, esp. due to the consequences for the people who could use a medical miracle. Though some who have undergone surgery have more hardware in their bodies than I do, we’re all on a spectrum, with an organic non-GMO human at one end and “something beyond human” at the other. A path has been laid out for decades in ways both calculated and spontaneous, conscious and unconscious — it continues to develop and draw attention, inspiring fear and awe as it accelerates towards an apotheosis.
If as I suspect we live in a multiverse, there may be countless futures, and those futures arrive by tiny steps. People have always been using tools to survive and thrive, including eyeglasses, hearing aids, canes, prosthetics, and pharmaceuticals. At the next level we have tools that become part of the body, or that modify the body (and the human experience) in a lasting sense: implants, pacemakers, grafts, transplants, and gene therapies. One way to consider this transformation is to view the human being as a Ship of Theseus. Imagine replacing your body parts with replicas as they wear out or become diseased over a span of many years, until no original parts are left.
This raises the question: is there a boundary that we can agree upon, beyond which someone is no longer the same person? Is that “something else” measurable, or could it be just an intuition, a vibe? Will there come a time when we can no longer regard humanity as one species — not as a regression to racism, but the recognition of a new “other” among us? The deconstruction of gender in recent years could be a preview of the controversies to come, esp. if people seek enhancements not just out of medical necessity, but to succeed at the game of life as they imagine it. We have already seen the widespread normalization of cosmetic surgery and body mods like tattoos and piercings. I’m not saying the slope must be slippery, but the slope exists, and it makes tons of money.
Belief systems about the physical realm are founded upon the metaphysical — in this light, the transhumanist movement can be seen as allopathic medicine taken to its logical extreme, by regarding morbidity and mortality as engineering problems. If the reality map, the metaphysical foundation, is based on an error, even if the research amasses valid data and makes logical deductions, the underlying error remains.
If you wonder where I’m at, to me it is perfectly consistent to view all phenomena as made of Consciousness, i.e., a dream in the mind of God. To employ the metaphor of a simulation, anyone not playing in god-mode must respect the game physics. Someone who thinks he understands ultimate reality would be wise to not jump off the roof to demonstrate the illusion of gravity! So far no one has offered me the cheat codes to fly like St. Joseph of Cupertino.
Systemic Obstacles to Wellness
A patient who thinks independently and takes a proactive role in the healing process will inevitably have to question the establishment’s cherished assumptions, which only hold sway due to gaslighting:
1) Trained experts are the authorities to whom laypeople should defer, always;
2) If a drug, device, or procedure was approved by the relevant regulatory body, that should assure you of its safety and efficacy in most cases;
3) Peer-reviewed studies reliably produce valid scientific knowledge;
4) The profit motive does not influence our options and decision-making adversely and should not cast doubt on the key assumptions above.
To engage with the medical system as the one in charge of your body takes diplomacy and diligence. Though I have medical library experience in my favor, I don’t pretend to have the same depth of knowledge as an MD or an RN. The onus is on me to back up my positions with reputable sources and to demonstrate that I actually know what I’m talking about. Regarding CV disease, my objections are unrelated to the surgery, for a radical intervention was called for to protect my life. What I question is reliance on meds as essential to treatment, and the logic behind the treatment goals.
In recent years there have been more dissident doctors calling for a reappraisal of the MIC’s drug protocol, esp. in light of studies indicating that the obsession with LDL cholesterol level is misplaced; hence disappointing outcomes in terms of longevity, not to mention patients harmed by statin side effects. The issues of insulin resistance and inflammation as drivers of CV disease are gaining visibility at last; though these risk factors are still not necessarily ultimate causes, they are reactions that lie nearer to the root of the problem.
From Framingham to Hunt 2: 60 Years Blaming the Wrong Culprit?
Would you be shocked to learn that in 1967 the sugar industry influenced the course of medical research for decades by funding a study published in the New England Journal of Medicine? This scandal was exposed only eight years ago. Imagine how much money is (has always been) at stake for the food and pharmaceutical industries. If it becomes common knowledge that sugar is the real culprit in heart disease (not to mention other chronic illnesses), the medical cookbooks will have to be rewritten.
Big Sugar's Influence on Medical Research
Given how corruption is baked into military procurement with billions flowing to the arms industry annually, why would it be any different for the medical field? While I can’t confirm that any doctors I know are colluding with Big Pharma, the incentives for playing along have always been there, for ex., when new drugs are being rolled out. Despite this, plenty of well-intentioned doctors and nurses do the best they know how within a misguided system run by psychopaths. The resemblance to how governments exploit the nobler impulses of their citizens for ignoble ends is hardly coincidental.

Muddling Through
Having spent weeks reading articles and watching videos on the various approaches to CV disease, I’ve concluded that if you search online you’ll find every aspect of the mainstream protocol debunked by some authority in the alternative health field. At this time I don’t think anyone has CV disease completely figured out. Whoever says there’s one easy answer to “clean out your arteries” is most likely oversimplifying. From my own experience I believe the way to start is by studying the mainstream position as it is currently taught. Then you may be better equipped to understand how an alternative modality works, if it works at all. (This assumes that the alternative in question operates in accord with the game physics and is not an attempt to evade causality in spacetime, i.e., magical thinking.)
Getting a handle on the decades-long process of atherosclerosis (aka hardening of the arteries) is no small feat. I may know more than I did two months ago about how our Rube Goldberg circulatory system malfunctions, but there is so much more, it boggles the mind. The illustration below is just an amuse-bouche:
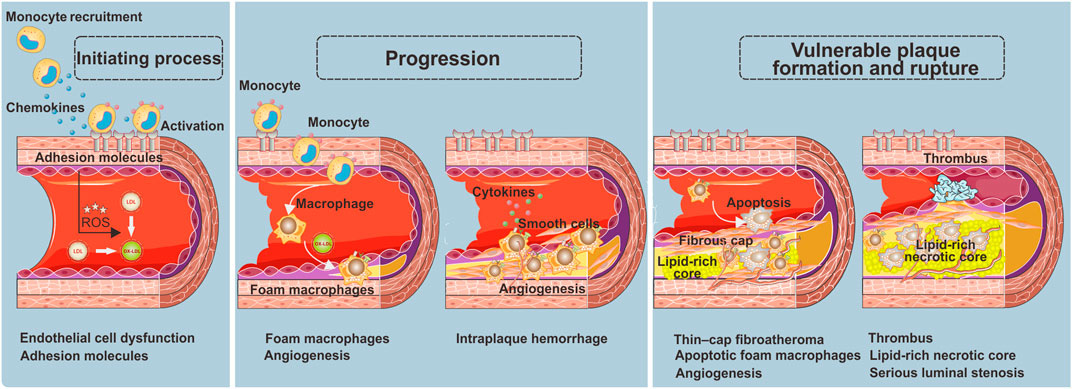
This is just an introductory diagram, representing just one of the possible chains of events, and only in the most localized sense, without the larger context.
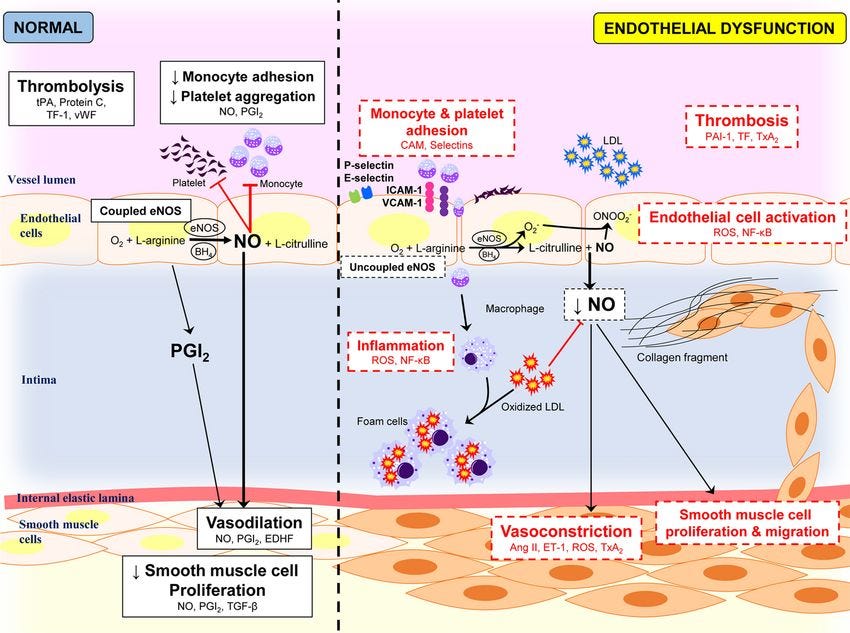
Here we have more detail, but without a full description of the components and the relationships between them. This is just to give you an impression of the complexity of this reality map. It doesn’t even mention apolipoprotein B (apo B) & lipoprotein (a), which have gained attention lately as independent risk factors. Notice the focus is always on how things go wrong in the body. Would it not also help to examine people without CV disease to figure out why their bodies don’t malfunction?
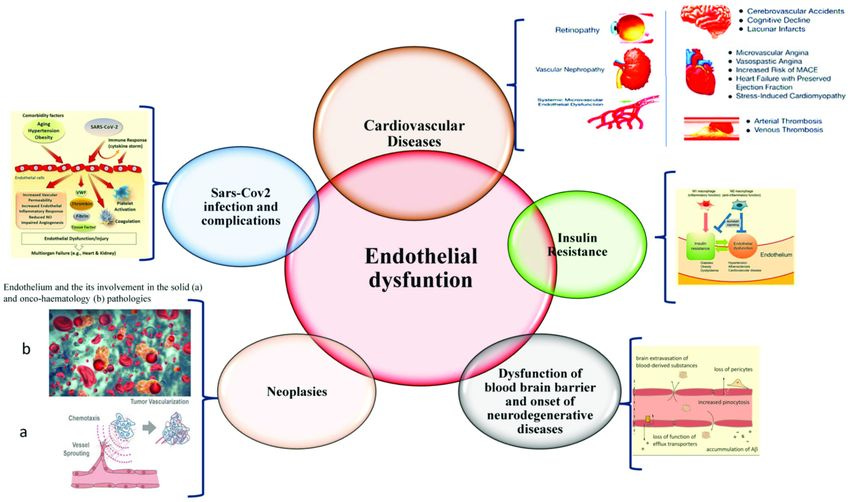
In this diagram a pattern has been detected regarding endothelial dysfunction, i.e., as a factor shared by different maladies — not the same as a common cause, but a step nearer to grasping the connections between degenerative diseases. For ex., there is a well-known linkage between diabetes and CV disease, so much that the former is seen as a risk factor for the latter. Ironically, statins, the most prescribed type of drug for lowering LDL cholesterol, can increase the risk of diabetes. Fancy that!
I’m not dispensing medical advice, but there are a few universally accepted lifestyle recommendations for those at risk for CV disease (we might as well say everyone):
Don’t smoke (duh!) — Personally I would not limit this to tobacco or to smoke from combustion only. If you must do drugs, try another route besides your lungs.
Lay off the processed foods! By now this should be as obvious as not smoking, but the lure of convenience is hard to resist. This goes for vegetarians as well.
Move that body! Players of “The Human Experience” have to get physical. This does not entail being a gym fanatic, but consistent effort over time will pay off.
Don’t stress out! Yeah, easier said than done. But this is the most mainstream layer between mind and body, where the metaphysical rubber meets the road. What if the real origins of chronic illness lie outside the physical realm?
Great writing my friend.